Management and Treatment of Abdominal Aortic Aneurysms
Aneurysmal disease can defined as a weakness in the wall of an artery which makes it more susceptible to rupture which is very often catastrophic as well as a nidus for arterial thromboembolic events. A ruptured abdominal aortic aneurysm and its inherent complications have the lives of several notable people in history including Albert Einstein, Lucille Ball, George C. Scott and Rodney Dangerfield. Initially there was not much to offer surgically to these patients with these lethal conditions. However with the advent of vascular surgery, open surgical repair was a viable option and saved many lives with this treatment regimen. However, due to the magnitude of the surgery, the prolonged and complicated perioperative course, it was quite an undertaking for an elderly population which may have other medical issues. Since that time and with the development of endovascular procedures, the treatment of abdominal aortic aneurysm have changed to procedures that are less invasive.
Screening:
Us Preventative Services Task Force recommends single screening ultrasound for abdominal aortic aneurysm in males aged 65-75 who have a history of tobacco use. It is unclear if screening is useful in women aged 65-75 who have smoked and they recommend against screening in woman who never smoked.
Repeat ultrasound should be performed in patients with aortic size greater than 3.0 cm. In these patients if aortic size is between 3-3.9 cm the ultrasound should be repeated every 3 years. If between 4.0- 4.4 every 2 years and if between 4.5- 5.4 cm every year. If greater than 5.4 cm should consider for elective repair.
Risk Factors:
Diagnosis:
Physical Examination:
A thorough abdominal examination may diagnose the presence of a pulsatile abdominal mass which may represent an enlarging AAA. The presence of an abdominal bruit may suggest turbulent flow which may occur with an aneurysm. The presence of pulsatile popliteal masses bilaterally may not diagnose a AAA directly but the presence of bilateral popliteal artery aneurysms may suggest an increased incidence of AAA. The presence of severe abdominal and back pain, flank pain and abdominal ecchymosis may suggest a leaking or ruptured AAA.
Abdominal Ultrasound:
This modality has become a standard as an initial screening study. It is noninvasive, does not expose the patient to radiation and can be an assessment tool in AAA surveillance. Limitations may occur secondary to body habitus and the presence of bowel gas. Abdominal Ultrasound can also be used in a emergent situation to determine the presence of free fluid which may suggest a leaking or ruptured AAA.
Abdominal CT scan:
An abdominal CT scan can be quite helpful in planning repair of the AAA. It an determine which patients are appropriate for endovascular repair versus open repair. This may be based on the length of the aortic neck, angulation or tortuosity of the iliac arteries. It is important to determine if an endovascular repair is feasible versus an open repair. It is also quite helpful in determining the presence of venous anomalies which might have horrendous implications if not determined prior to an open operative repair. An abdominal CT scan may also determine the presence of a leaking or ruptured AAA by the presence of retroperitoneal blood or intraperitoneal bleeding. But from a management standpoint, this should be preclude a patient from going to operating room.
SAAVE Act:
The Screening Abdominal Aortic Aneurysm Very Efficiently Act (SAAVE Act): At risk patients entering Medicare can receive a free one time screening study for AAA. The Act allows for screening as part of the “Welcome to Medicare Physical Exam”, officially known as an Initial Preventative Physical Examination. To be covered by Medicare, the AAA screening must be ordered at the time of Welcome to Medical Physical Exam and must be performed within one year of Medicare enrollment. AAA screening for at risk patients includes those with a history of smoking, older than 60 years of age, family history of AAA, Hypertension, elevated cholesterol, COPD, coronary artery disease and prior CABG.
Treatment Options:
The treatment options of repair of abdominal aortic aneurysms have changed significantly over the last 2 decades. Twenty years ago, the standard treatment of abdominal aortic aneurysm was open repair with its inherent perioperative risks and complications. With that treatment modality, there was always a subset of patients who were considered to be too frail with other comorbidities and medical problems to undergo an operation of that magnitude. At that time there was not much to offer them. However with the advent of endovascular procedures and the use of Aortic stent grafts, these patients have options in a procedure that can now be performed with local anesthesia and IV sedation and these patients can be discharged home within 24 hours. It is to the point now where aortic stent grafts have become the standard on how to treat these patients.
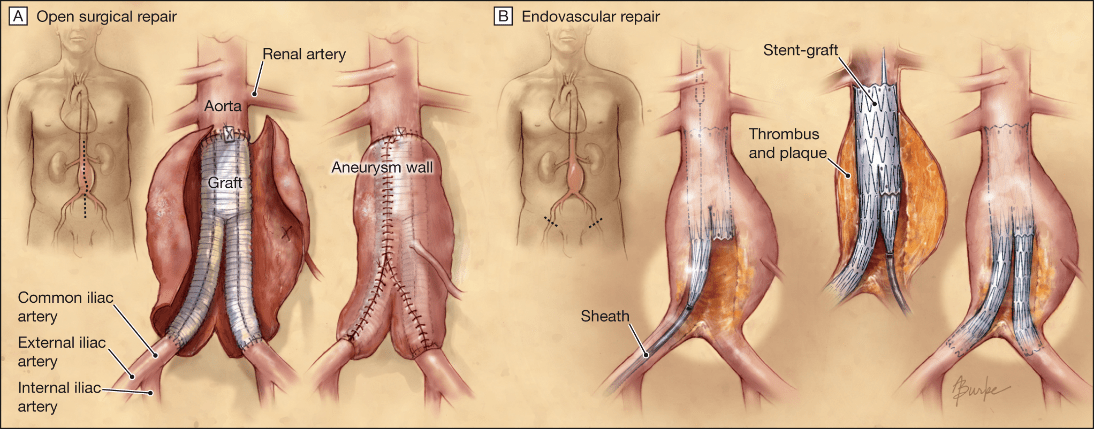
Comparison of open stent graft repair versus stent grafts. The stent graft can be performed with local anesthesia and intravenous sedation. The instrumentation and operative team are standing by and available if a stent graft cannot be placed and an open procedure is necessary. In terms of hospital stay, the average stent graft patient is in the hospital for 24-48 hours as opposed to open aneurysm repair stay of 5-7 days.
